Mechanical ventilation is a critical skill area for every nurse, especially those preparing for the NCLEX or working in critical care. As a registered nurse (RN nurse), understanding ventilator settings can be the difference between safe patient care and dangerous complications. This guide breaks down key ventilator settings in a simplified way, perfect for nursing students and those using a nursing bundle for exam prep.
Why Ventilator Settings Matter for Nurses
Patients on ventilators are often unstable, with conditions such as ARDS, COPD exacerbations, trauma, or post-surgical complications. Nurses are responsible for monitoring these patients, recognizing abnormal findings, and communicating with the healthcare team.
On the NCLEX, ventilator questions test your ability to prioritize safety, interpret alarms, and identify complications like barotrauma or hypoxemia.
Key Ventilator Settings Explained
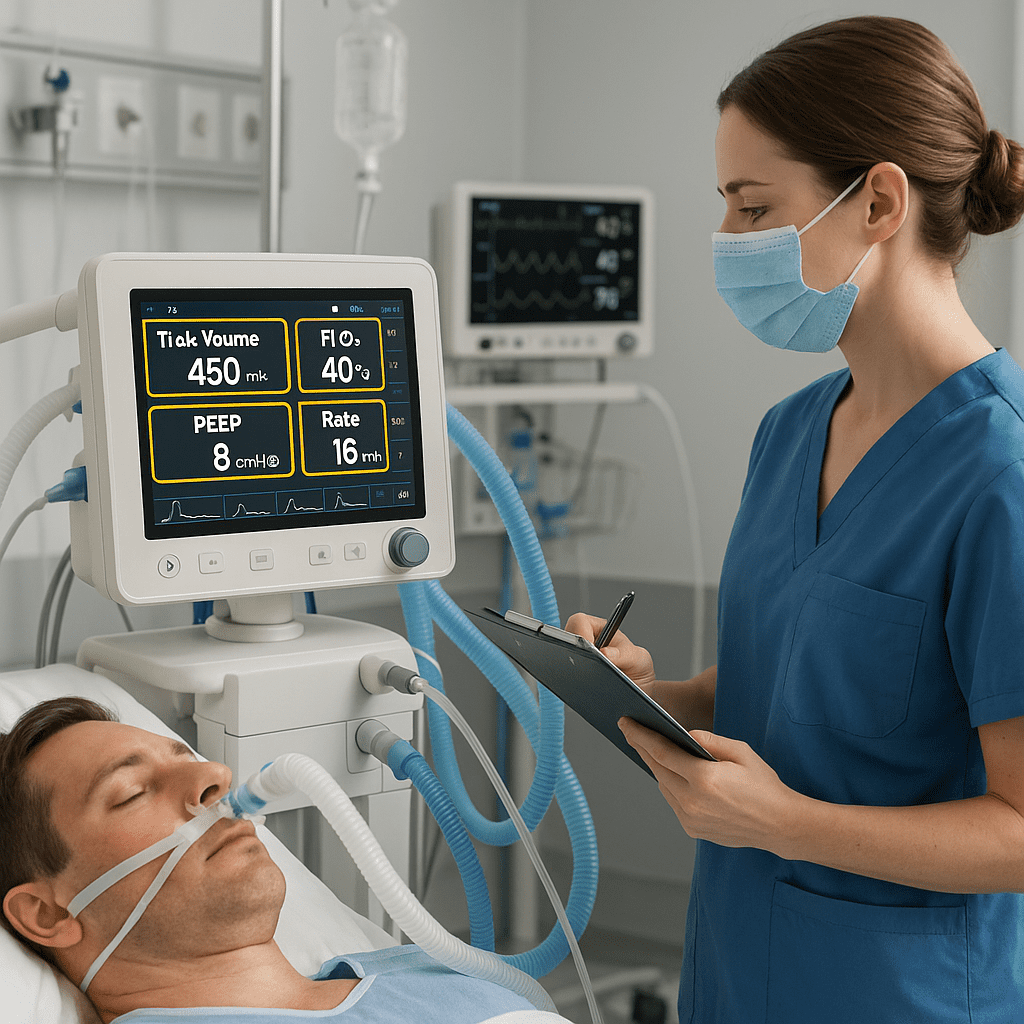
1. Tidal Volume (VT)
- Definition: The amount of air delivered with each breath (measured in mL).
- Nursing Notes: Usually set at 6–8 mL/kg of ideal body weight. Too high can cause lung injury; too low may cause hypoventilation.
2. Respiratory Rate (RR)
- Definition: Number of breaths delivered per minute.
- Nursing Notes: Normal is 12–20, but may be higher in ARDS to blow off CO₂. Monitor for hyperventilation and respiratory alkalosis.
3. FiO₂ (Fraction of Inspired Oxygen)
- Definition: Percentage of oxygen delivered to the patient.
- Nursing Notes: Usually starts at 100% during intubation, then titrated down. Goal is to keep O₂ sat > 90% while minimizing oxygen toxicity.
4. PEEP (Positive End-Expiratory Pressure)
- Definition: Pressure applied at the end of exhalation to keep alveoli open.
- Nursing Notes: Improves oxygenation in ARDS, but high levels may cause hypotension or pneumothorax.
5. Mode of Ventilation
- Assist-Control (AC): Every breath is supported with preset volume/pressure. Best for very sick patients, but can lead to respiratory alkalosis.
- SIMV (Synchronized Intermittent Mandatory Ventilation): Provides set breaths but allows spontaneous breathing. Used during weaning.
- Pressure Support Ventilation (PSV): Patient initiates breaths, and the vent assists. Encourages independence.
Nursing Priorities with Ventilator Settings
As a nurse or RN nurse, your key responsibilities include:
- Monitoring vital signs, ABGs, and SpO₂.
- Checking for signs of hypoxemia, hypercapnia, or barotrauma.
- Responding to ventilator alarms promptly.
- Positioning the patient (often semi-Fowler’s).
- Providing oral care to prevent ventilator-associated pneumonia (VAP).
NCLEX Tip: Ventilator Alarms
- High-pressure alarm: Secretions, kinked tubing, coughing, biting the tube.
- Low-pressure alarm: Disconnection, leak, or cuff deflation.
👉 On the NCLEX, never silence the alarm without assessing the patient first.
Final Thoughts
Ventilator settings may seem intimidating, but with practice, nurses can master them. For NCLEX prep, focus on knowing what each setting does, nursing priorities, and how to respond to alarms. Using a nursing bundle can simplify these complex concepts into easy-to-follow charts, making you confident both for exams and in real-life practice as a registered nurse.
❓ FAQ: Ventilator Settings Nurses Must Understand
For NCLEX and clinical practice, nurses must understand tidal volume (VT), FiO₂, PEEP, rate, and modes (AC, SIMV, CPAP, BiPAP). These affect oxygenation, ventilation, and patient safety.
Oxygenation is controlled mainly by FiO₂ and PEEP.
Ventilation is controlled by tidal volume (VT) and respiratory rate (RR).
Nurses must monitor both to ensure adequate gas exchange.
PEEP prevents alveolar collapse at the end of expiration, improving oxygenation. However, high PEEP can reduce cardiac output and risk barotrauma, so nurses must monitor blood pressure and lung compliance.
Monitor respiratory rate, SpO₂, ABGs, and lung sounds.
Assess for synchrony with the ventilator (fighting the vent).
Watch for complications like ventilator-associated pneumonia (VAP) or barotrauma.
Check the patient first, not just the machine.
Ensure the airway is patent (check for kinks, secretions, or disconnection).
If unresolved quickly, disconnect and manually bag with 100% oxygen until the issue is corrected.
Yes ✅. The NCLEX often tests which setting to adjust first or how to prioritize nursing interventions when a ventilated patient shows abnormal ABGs or distress.