STEMI and NSTEMI help nurses catch cardiac problems early and deliver lifesaving treatment fast. In this guide, we’ll break down what these two heart attacks look like, how to tell them apart, and most importantly, what actions to take next.
🫀 What’s a STEMI and What’s an NSTEMI?
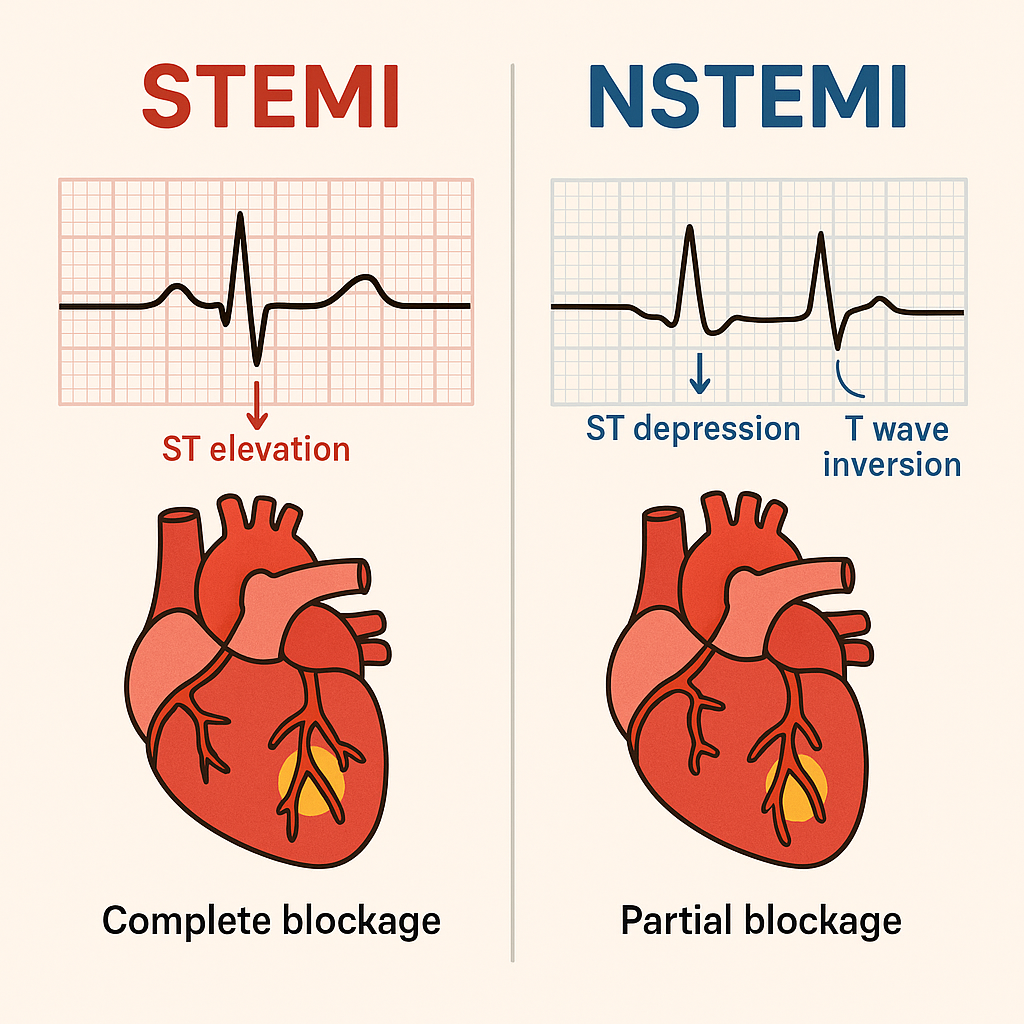
Both STEMI and NSTEMI indicate that the heart muscle isn’t getting enough oxygen because of a blocked coronary artery. However, they appear differently on an EKG and require slightly different interventions.
STEMI means:
✅ ST-Segment Elevation Myocardial Infarction
✅ Complete blockage of a coronary artery
✅ Rapid heart muscle death
✅ Requires immediate reperfusion — usually in the cath lab within minutes
NSTEMI means:
✅ Non-ST-Segment Elevation Myocardial Infarction
✅ Partial blockage of a coronary artery
✅ Some damage to heart tissue
✅ No ST elevation on EKG — but other ischemic signs appear
✅ Requires urgent, but not immediate, treatment
In short, both are dangerous, yet STEMI is more time-sensitive and life-threatening.
🩺 How a Heart Attack Happens
To understand these differences better, let’s review how a heart attack actually develops:
- Plaque rupture: A cholesterol plaque in a coronary artery tears open.
- Clot formation: A blood clot quickly forms at the tear site.
- Blood flow interruption: If fully blocked → STEMI; if partially blocked → NSTEMI.
- Oxygen deprivation: The heart muscle starts to die without oxygen.
- EKG changes: Damaged cardiac cells cause abnormal electrical activity.
Therefore, early recognition and rapid action are critical.
📊 Key EKG Changes in STEMI
A classic STEMI has distinct and urgent EKG signs:
✅ 1. ST-Segment Elevation
This is the most alarming finding.
Look for:
- ST elevation in two or more contiguous leads (leads viewing the same heart area).
- Elevation >1 mm in limb leads or >2 mm in precordial leads.
For example:
- V1–V4 → Anterior STEMI
- II, III, aVF → Inferior STEMI
- I, aVL, V5–V6 → Lateral STEMI
✅ 2. Reciprocal Changes
In contrast, you’ll often see ST depression in opposite leads.
For instance: an Inferior STEMI often shows depression in leads I and aVL.
✅ 3. Possible Pathological Q Waves
Later on, deep Q waves may appear, signaling irreversible muscle death.
⚠️ Red Flag Signs for STEMI
Clinically, watch for these urgent warning signs:
- New ST elevation matching chest pain
- Crushing, radiating chest pain (“elephant on chest”)
- Pain spreading to arm or jaw
- Pallor, diaphoresis, anxiety
- Hypotension or signs of shock
👉 Therefore, act fast: Call the rapid response team, alert cardiology, and prepare for the cath lab immediately.
📊 Key EKG Changes in NSTEMI
Unlike STEMI, NSTEMI doesn’t produce a clear ST elevation — but other subtler clues appear:
✅ 1. ST-Segment Depression
Usually horizontal or downsloping ST depression in two or more leads.
This indicates ischemia, meaning the heart muscle is starved but not yet dead.
✅ 2. T-Wave Inversions
Deep inverted T waves, especially in leads V2–V6, suggest areas of reduced oxygenation.
✅ 3. No Q Waves (Usually)
Because there’s no full-thickness myocardial damage like in STEMI.
Altogether, these changes still signal danger — so nurses must respond rapidly.
⚡ STEMI vs. NSTEMI Cheat Sheet
| Feature | STEMI | NSTEMI |
|---|---|---|
| ST Elevation | Yes, in contiguous leads | No |
| ST Depression | Reciprocal only | Common |
| T-Wave Inversion | Possible | Common |
| Q Waves | Possible | Rare |
| Blockage | Complete | Partial |
| Damage | Full-thickness | Partial-thickness |
| Treatment | Immediate reperfusion (PCI/fibrinolytics) | PCI, but less urgent |
In summary, both require quick nursing assessment — but STEMI always comes first in priority.
🏥 Nursing Actions for Suspected Heart Attack
When you suspect STEMI or NSTEMI, act methodically:
1️⃣ Stay with the patient – Never leave them unattended.
2️⃣ Call for help immediately – Activate your rapid response or chest pain protocol.
3️⃣ Get a 12-lead EKG promptly – Repeat as needed; changes can evolve quickly.
4️⃣ Administer oxygen if necessary – Only if O₂ saturation < 90%.
5️⃣ Obtain vital signs – Watch for hypotension or arrhythmias.
6️⃣ Establish IV access – Preferably two large-bore IVs.
7️⃣ Prepare essential medications:
- Aspirin (chewable)
- Nitroglycerin (unless hypotensive)
- Morphine (if pain persists)
8️⃣ Notify cardiology right away – Prepare for cath lab if STEMI confirmed.
Meanwhile, keep the patient calm and continuously reassess for new symptoms.
📌 What NOT to Miss
🚫 Don’t ignore vague symptoms: Older adults, women, and diabetics may have mild or atypical presentations.
🚫 Don’t delay the first EKG: It must be completed within 10 minutes of chest pain onset.
🚫 Don’t give nitro if hypotensive or if you suspect a right ventricular infarct (ST elevation in V4R).
Remember, a few minutes of delay can change the patient’s outcome dramatically.
🗂️ Extra: STEMI Mimics Every Nurse Should Know
Sometimes, other conditions can look like a STEMI but aren’t. Knowing these can prevent misdiagnosis:
- Pericarditis: Diffuse ST elevation without reciprocal depression.
- Early repolarization: Common in healthy young adults.
- Left Bundle Branch Block (LBBB): Wide QRS and atypical ST changes.
- Ventricular aneurysm: Persistent ST elevation due to old MI scar.
If uncertain, always consult cardiology for a second opinion — sooner rather than later.
🗝️ Key Takeaway
Ultimately, distinguishing between STEMI and NSTEMI helps nurses provide faster, safer, and smarter care. By recognizing EKG changes, responding immediately, and following your facility’s chest pain protocol, you protect your patient’s heart — and possibly save their life.