Sodium imbalances are among the most dangerous electrolyte disorders in clinical practice. However, what is often even more dangerous than hyponatremia itself is correcting it too quickly. Rapid sodium correction can lead to Osmotic Demyelination Syndrome (ODS) — a devastating neurologic complication. For every nurse, especially the ICU registered nurse (RN nurse), understanding this condition is essential for safe nursing care and strong NCLEX performance.
Correct chronic hyponatremia slowly — rapid sodium correction can cause irreversible brain damage known as Osmotic Demyelination Syndrome.
Understanding Sodium and Brain Adaptation
Normal sodium level:
135–145 mEq/L
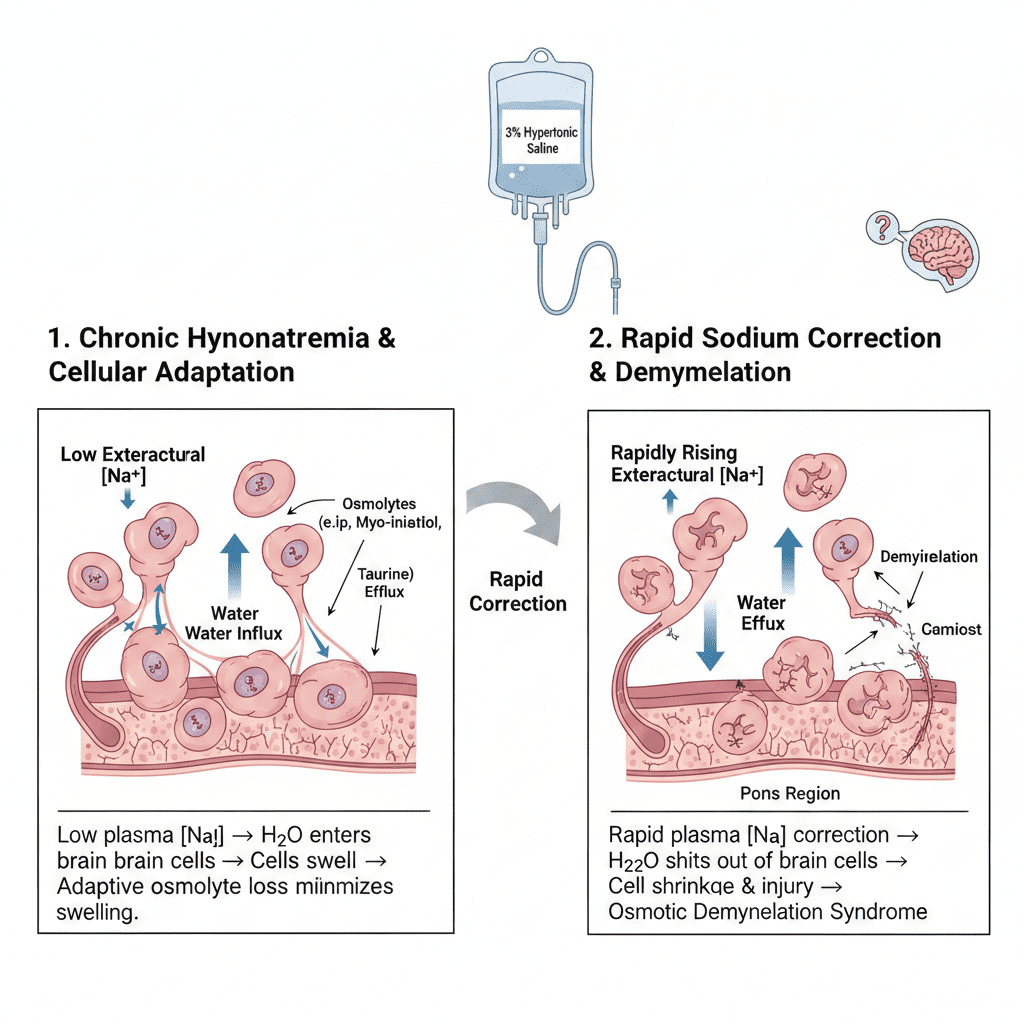
Sodium regulates extracellular fluid balance. When sodium levels drop (hyponatremia), water shifts into brain cells, causing cerebral edema.
The Brain’s Adaptive Mechanism
If hyponatremia develops slowly (chronic):
- Brain cells adapt by losing osmolytes
- Intracellular solutes decrease
- Swelling reduces over time
This adaptation protects against severe edema — but it creates danger if sodium is corrected too quickly.
For the RN nurse, timing matters.
What Happens During Rapid Sodium Correction?
When sodium is rapidly increased:
1️⃣ Serum osmolality rises quickly
2️⃣ Water shifts out of brain cells
3️⃣ Cells shrink abruptly
4️⃣ Myelin sheaths become damaged
This leads to Osmotic Demyelination Syndrome (ODS), formerly called central pontine myelinolysis.
What Is Osmotic Demyelination Syndrome?
Osmotic Demyelination Syndrome is a neurologic disorder caused by rapid correction of chronic hyponatremia.
It involves:
- Demyelination of nerve cells
- Most commonly in the pons
- Irreversible neurologic injury in severe cases
This is a high-yield NCLEX concept.
Who Is at Highest Risk?
The nurse should be especially cautious in patients with:
- Chronic hyponatremia (>48 hours)
- Alcohol use disorder
- Malnutrition
- Liver disease
- SIADH
- Severe electrolyte disturbances
These patients are frequently seen in critical care and medical-surgical nursing units.
Safe Sodium Correction Guidelines
For chronic hyponatremia:
- Increase sodium no more than 8–10 mEq/L in 24 hours
- No more than 18 mEq/L in 48 hours
Slower correction is safer.
The registered nurse must:
- Monitor serum sodium every 2–4 hours in critical cases
- Carefully regulate hypertonic saline infusions
- Use infusion pumps (never free-flow)
Overcorrection can occur even unintentionally.
Symptoms of Osmotic Demyelination Syndrome
Symptoms often appear 2–6 days after correction.
They include:
- Dysarthria
- Dysphagia
- Confusion
- Quadriparesis
- “Locked-in” syndrome
- Decreased level of consciousness
Unlike cerebral edema from hyponatremia, ODS symptoms may be delayed.
The RN nurse must monitor neurologic status closely even after sodium appears normalized.
Hypertonic Saline and Nursing Considerations
3% saline may be used in severe symptomatic hyponatremia (seizures, coma).
Nursing priorities:
- Continuous cardiac monitoring
- Frequent sodium checks
- Strict intake/output monitoring
- Assess for neurologic changes
- Double-check infusion rates
A structured electrolyte nursing bundle prevents complications.
Why Acute vs Chronic Hyponatremia Matters
Acute Hyponatremia (<48 hours)
- Brain has not adapted
- Faster correction may be tolerated
Chronic Hyponatremia (>48 hours)
- Brain has adapted
- Rapid correction causes demyelination
On the NCLEX, the question often hinges on duration.
Always determine how long hyponatremia has been present.
The Role of Desmopressin (DDAVP)
Sometimes sodium corrects too quickly due to:
- Water diuresis
- Resolution of SIADH
- Overcorrection with hypertonic saline
Providers may administer desmopressin to:
- Slow sodium rise
- Prevent further correction
The registered nurse must understand the rationale behind this intervention.
Nursing Bundle for Safe Sodium Management
A safety-focused nursing bundle includes:
1️⃣ Determine acute vs chronic status
2️⃣ Monitor sodium levels frequently
3️⃣ Avoid rapid IV fluid adjustments
4️⃣ Use infusion pumps
5️⃣ Perform frequent neurologic assessments
6️⃣ Educate patient and family
Prevention is the only true treatment for ODS.
NCLEX High-Yield Review
- Chronic hyponatremia must be corrected slowly
- No more than 8–10 mEq/L increase in 24 hours
- Rapid correction → Osmotic Demyelination Syndrome
- ODS causes neurologic deficits
- Monitor sodium frequently
- 3% saline requires close monitoring
If a malnourished patient develops neurologic deficits days after sodium correction, suspect ODS.
Integrating Sodium Safety into Nursing Practice
For the experienced RN nurse, managing sodium imbalances requires precision, vigilance, and deep pathophysiologic understanding.
Mastering this topic improves:
- Critical care skills
- IV fluid management
- Neurologic assessment
- Electrolyte interpretation
- NCLEX exam readiness
Safe sodium correction reflects advanced clinical judgment in modern nursing practice.
Final Thoughts
Hyponatremia can be life-threatening — but correcting it too quickly can be even more devastating. Osmotic Demyelination Syndrome is a preventable complication that underscores the importance of careful electrolyte management.
For every nurse and registered nurse, understanding the risks of rapid sodium correction is essential for delivering safe, evidence-based nursing care and excelling on the NCLEX.
Slow correction saves neurons. Precision saves lives.