A High-Yield NCLEX Guide for the Nurse, Registered Nurse, and RN Nurse
Pacemaker malfunction is identified on ECG by failure to pace, failure to capture, or failure to sense — and rapid recognition by the nurse can prevent hemodynamic collapse.
For every nurse, registered nurse, and RN nurse, recognizing pacemaker malfunction on ECG is a life-saving skill. Pacemakers are designed to maintain adequate heart rate and cardiac output, but when they malfunction, patients may quickly deteriorate.
This guide provides a clear, NCLEX-focused breakdown of pacemaker malfunction patterns, ECG recognition tips, and a structured nursing bundle approach.
Understanding Normal Pacemaker Function
Before identifying malfunction, the nurse must recognize normal pacing patterns.
On ECG, a functioning pacemaker shows:
- Small vertical pacer spikes
- Spike followed by appropriate depolarization
- Atrial spike → P wave
- Ventricular spike → Wide QRS complex
In ventricular pacing, the QRS is typically wide because the impulse originates outside the normal conduction pathway.
For NCLEX success and safe nursing practice, always ask:
Does every spike produce a beat?
The 3 Major Pacemaker Malfunctions
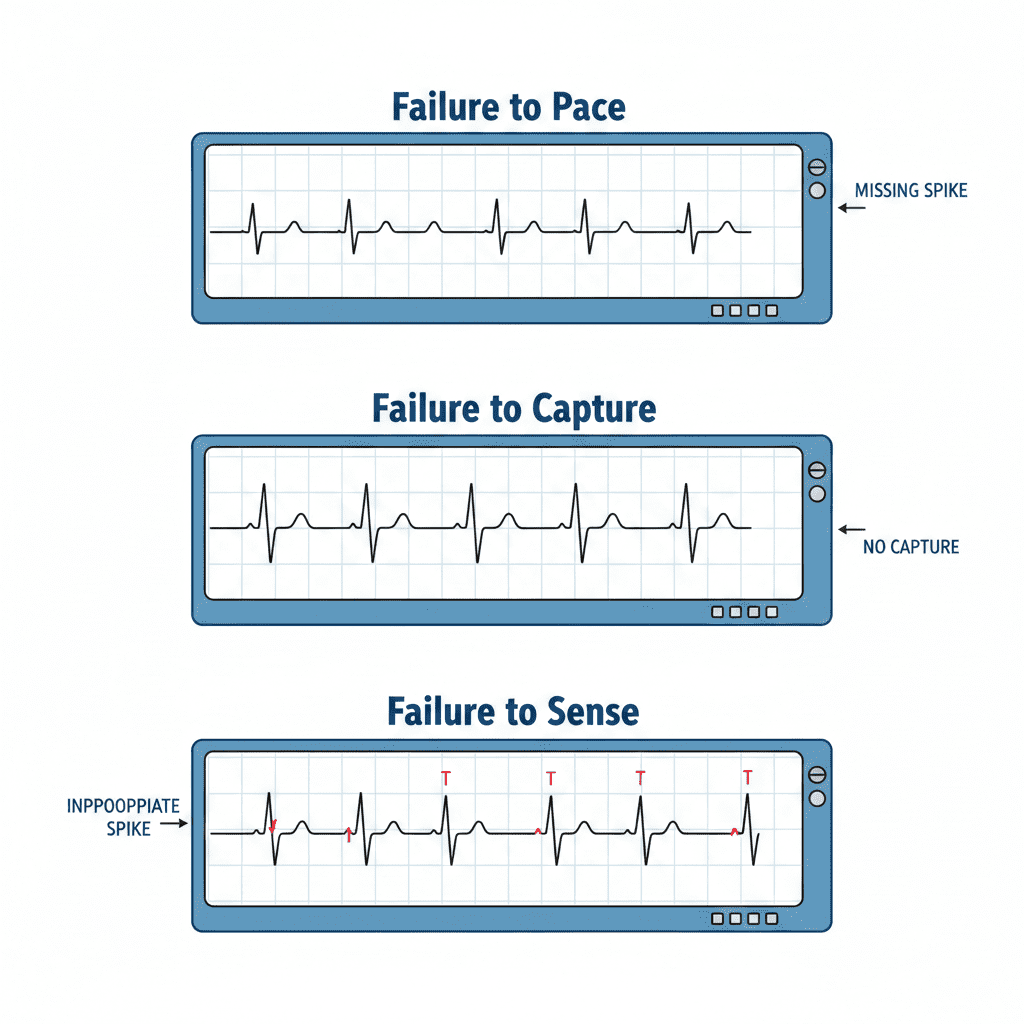
1️⃣ Failure to Pace
What You See on ECG:
- No pacer spikes when heart rate drops below set rate
- Unexpected bradycardia
- Long pauses
This means the pacemaker is not firing.
Clinical Causes:
- Battery depletion
- Lead disconnection
- Generator failure
Nursing Priority:
- Assess patient immediately
- Check pulse and blood pressure
- Apply oxygen
- Notify provider
- Prepare for temporary pacing if unstable
For the RN nurse, this is a potential emergency.
2️⃣ Failure to Capture
What You See on ECG:
- Pacer spike present
- No P wave or QRS after spike
The pacemaker fires — but the myocardium does not respond.
This is the most commonly tested malfunction on NCLEX.
You will see: PacerSpike→(NoQRS)=FailuretoCapturePacer Spike → (No QRS) = Failure to CapturePacerSpike→(NoQRS)=FailuretoCapture
Common Causes:
- Lead displacement
- Fibrosis at lead tip
- Electrolyte imbalance (especially hyperkalemia)
- Acidosis
Nursing Actions:
- Assess hemodynamic stability
- Check electrolytes
- Reposition patient (if early post-op)
- Prepare for pacing threshold adjustment
Failure to capture can rapidly reduce cardiac output — every nurse must treat it as urgent.
3️⃣ Failure to Sense
What You See on ECG:
- Pacer spikes appear randomly
- Spikes may occur during intrinsic beats
- Spikes may fall in dangerous periods (R-on-T risk)
This occurs when the pacemaker does not detect the patient’s own cardiac activity.
You may see spikes inappropriately placed. IntrinsicQRS+RandomSpike=FailuretoSenseIntrinsic QRS + Random Spike = Failure to SenseIntrinsicQRS+RandomSpike=FailuretoSense
Causes:
- Lead displacement
- Oversensing/undersensing
- Electrical interference
Nursing Concern:
Improper sensing can trigger dangerous arrhythmias.
Immediate assessment by the registered nurse is required.
Quick Comparison Table for Nurses
| Malfunction | Spike Present? | QRS After Spike? | Rhythm Pattern |
|---|---|---|---|
| Failure to Pace | No | No | Bradycardia |
| Failure to Capture | Yes | No | Missed beats |
| Failure to Sense | Yes | Yes (but inappropriate timing) | Irregular pacing |
This table format is commonly tested on NCLEX exams.
Hemodynamic Assessment: Always Assess the Patient First
The most important nursing principle:
Treat the patient, not just the monitor.
Signs of instability:
- Hypotension
- Altered mental status
- Chest pain
- Syncope
- Weak pulse
An unstable patient with pacemaker malfunction may require:
- Emergency transcutaneous pacing
- Atropine (if bradycardic and indicated)
- Rapid response activation
Pacemaker Nursing Bundle
A structured cardiac nursing bundle for pacemaker patients includes:
1. Continuous Telemetry Monitoring
2. Daily Rhythm Interpretation
3. Lead Position Assessment (post-op patients)
4. Electrolyte Monitoring
5. Incision Site Assessment
6. Patient Education
This bundle improves early recognition and patient safety.
Electrolytes and Pacemaker Function
Electrolyte imbalances are a major cause of capture failure.
Especially monitor:
- Potassium
- Magnesium
- Calcium
Hyperkalemia is particularly dangerous in paced patients.
Every RN nurse in telemetry or ICU should monitor labs closely.
Post-Implant Nursing Considerations
For newly implanted pacemakers:
- Restrict arm movement (per protocol)
- Monitor for lead displacement
- Check for diaphragmatic pacing (hiccups)
- Inspect incision for infection
Infection or lead movement can lead to malfunction.
NCLEX-Style Clinical Scenario
A patient with a ventricular pacemaker shows pacer spikes with no QRS complexes. The patient reports dizziness and BP is 86/50.
What is occurring?
→ Failure to capture.
Priority action?
→ Assess patient and prepare for pacing intervention.
The NCLEX emphasizes patient safety and prioritization.
Advanced Insight for the Registered Nurse
Pacemaker malfunction can sometimes mimic other arrhythmias.
For example:
- Failure to capture may resemble sinus arrest
- Failure to sense may resemble ventricular ectopy
Always look for pacer spikes.
If spikes are present, think pacemaker-related issue.
Documentation Tips for the Nurse
Document:
- Type of pacemaker (if known)
- Mode (e.g., VVI, DDD if available)
- Presence or absence of spikes
- Patient symptoms
- Vital signs
- Interventions performed
- Provider notification
Accurate documentation protects the nurse and supports quality care.
Key Takeaways for NCLEX and Nursing Practice
✔️ Failure to pace = no spikes
✔️ Failure to capture = spike but no QRS
✔️ Failure to sense = spikes at wrong times
✔️ Always assess hemodynamic stability
✔️ Electrolytes matter
✔️ Treat the patient first
Pacemaker malfunction recognition is a critical skill for every nurse, registered nurse, and RN nurse working in cardiac, telemetry, ICU, or emergency settings.
Early recognition can prevent:
- Syncope
- Cardiogenic shock
- Cardiac arrest
Final Thoughts for the RN Nurse
Pacemakers are life-sustaining devices — but they are not failproof.
Your ability as a nurse to rapidly interpret ECG patterns, implement a cardiac nursing bundle, and escalate care appropriately can mean the difference between stability and collapse.
In cardiac nursing, vigilance saves lives.