Hyperkalemia is one of the most dangerous electrolyte emergencies in clinical practice. For any nurse, especially an ICU or telemetry registered nurse (RN nurse), recognizing the ECG progression of hyperkalemia can mean the difference between rapid intervention and cardiac arrest. Because potassium disorders are heavily tested on the NCLEX, mastering ECG changes associated with rising potassium levels is essential for safe nursing practice.
Peaked T waves are the earliest ECG sign of hyperkalemia — without rapid treatment, progression can lead to widened QRS, ventricular fibrillation, and cardiac arrest.
Normal Potassium Levels
Normal serum potassium:
3.5–5.0 mEq/L
Potassium plays a critical role in:
- Resting membrane potential
- Cardiac conduction
- Muscle contraction
- Nerve impulse transmission
Even small increases can destabilize cardiac electrical activity.
Why Hyperkalemia Affects the Heart
Potassium regulates the electrical gradient across myocardial cell membranes.
When potassium rises:
- Resting membrane potential becomes less negative
- Cells depolarize more easily
- Conduction slows
- Repolarization changes
This creates progressive ECG abnormalities.
For the RN nurse, understanding this cellular mechanism strengthens rhythm interpretation skills.
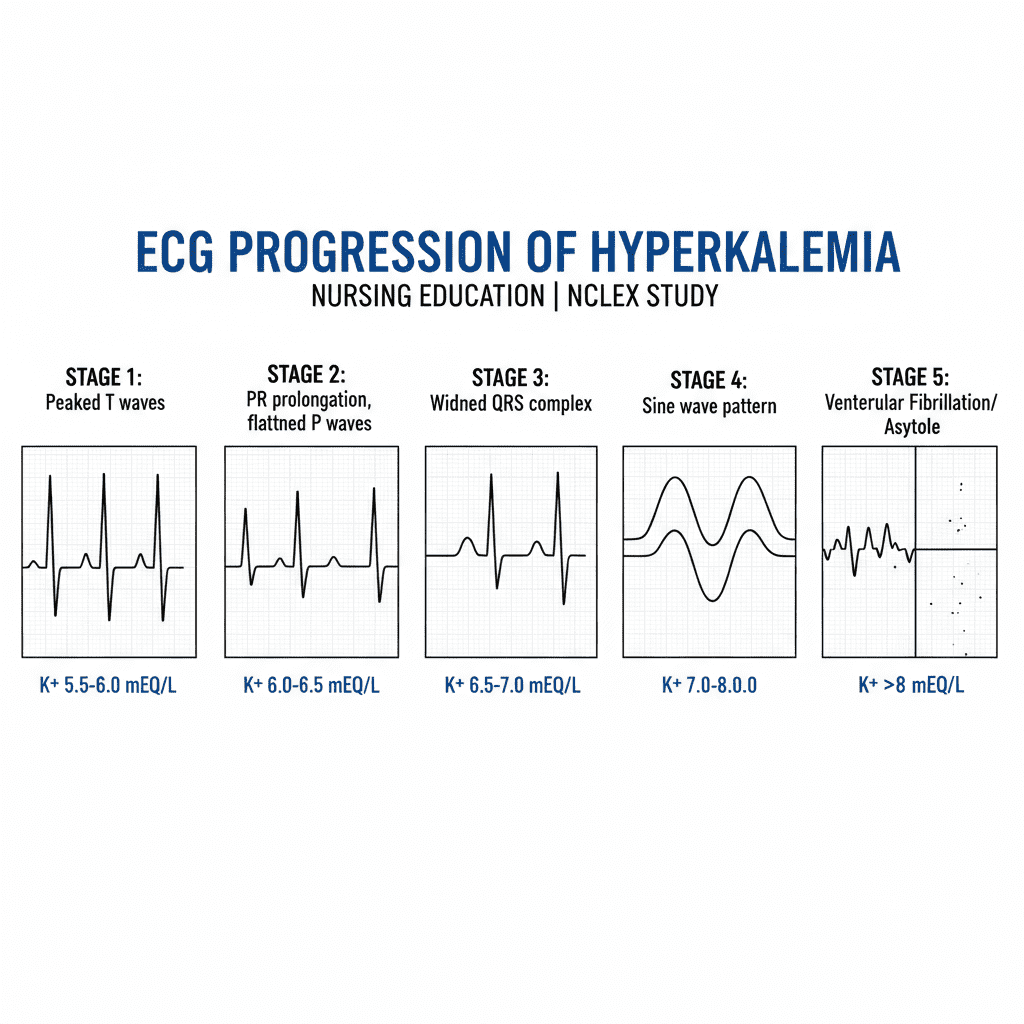
Stage 1: Peaked T Waves (Early Hyperkalemia)
Potassium: ~5.5–6.5 mEq/L
ECG Changes:
- Tall, narrow, peaked T waves
- Best seen in precordial leads
This is the earliest and most classic sign — a frequent NCLEX question.
At this stage, patients may be asymptomatic.
The nurse must notify the provider immediately and anticipate treatment.
Stage 2: PR Prolongation and P Wave Flattening
Potassium: ~6.5–7.5 mEq/L
ECG Changes:
- Prolonged PR interval
- Flattened P waves
- Possible atrial conduction delay
Atrial myocardium becomes suppressed before ventricular myocardium.
The registered nurse should increase monitoring frequency at this point.
Stage 3: QRS Widening
Potassium: ~7.0–8.0 mEq/L
ECG Changes:
- Widened QRS complex
- Slowed ventricular conduction
- Loss of P waves
This signals severe electrical instability.
At this stage, hyperkalemia becomes life-threatening.
Immediate intervention is required.
Stage 4: Sine Wave Pattern
Potassium: >8.0 mEq/L
ECG Changes:
- QRS merges with T wave
- “Sine wave” appearance
- No distinct P waves
This is a pre-arrest rhythm.
The RN nurse must activate emergency response protocols.
Final Progression: Ventricular Fibrillation or Asystole
Without treatment, hyperkalemia may lead to:
- Ventricular fibrillation
- Pulseless ventricular tachycardia
- Asystole
- Cardiac arrest
This progression may occur rapidly.
Recognition saves lives.
Causes of Hyperkalemia
Common causes include:
- End-stage renal disease
- Acute kidney injury
- Potassium-sparing diuretics
- ACE inhibitors
- Tissue breakdown (rhabdomyolysis, burns)
- Metabolic acidosis
For the nurse, renal failure patients are highest risk.
Emergency Treatment Overview
Treatment follows a structured priority approach.
1️⃣ Stabilize the Cardiac Membrane
- IV calcium gluconate
This does NOT lower potassium — it stabilizes the myocardium.
2️⃣ Shift Potassium Into Cells
- Insulin + dextrose
- Sodium bicarbonate (if acidotic)
- Albuterol (beta-agonist)
These provide temporary correction.
3️⃣ Remove Potassium from the Body
- Loop diuretics
- Potassium binders
- Dialysis (most effective in renal failure)
The registered nurse must anticipate rapid treatment orders.
Nursing Bundle for Hyperkalemia Management
A structured hyperkalemia nursing bundle includes:
1️⃣ Continuous cardiac monitoring
2️⃣ STAT potassium level verification
3️⃣ IV access confirmation
4️⃣ Emergency medication preparation
5️⃣ Frequent vital sign monitoring
6️⃣ Documentation of ECG progression
7️⃣ Preparation for possible ACLS intervention
Standardized response improves outcomes.
Clinical Scenario (NCLEX Style Thinking)
A dialysis patient presents with weakness and peaked T waves.
What is the priority?
→ Administer IV calcium gluconate.
The NCLEX frequently tests recognition of ECG progression before full arrest occurs.
Why Hyperkalemia Is So Dangerous
Unlike many electrolyte disorders:
- Symptoms may be minimal
- ECG changes can progress rapidly
- Cardiac arrest may occur suddenly
The RN nurse must treat ECG changes — not just lab values.
Hyperkalemia in End-Stage Renal Disease
Dialysis patients are at constant risk.
Missed dialysis sessions can cause:
- Severe potassium elevation
- Rapid ECG deterioration
- Sudden cardiac death
Patient education is a key nursing responsibility.
Key ECG Memory Tool for Nurses
Think of the progression as:
T → P → QRS → Sine → Silence
- Peaked T waves
- Prolonged PR
- Wide QRS
- Sine wave
- Cardiac silence
This progression is frequently emphasized on the NCLEX.
Nursing Assessment Priorities
The registered nurse should:
- Assess telemetry trends
- Compare prior ECGs
- Monitor potassium trends
- Check renal function
- Assess muscle weakness
- Review medications
Early recognition is the difference between intervention and resuscitation.
NCLEX High-Yield Review
- Peaked T waves are earliest sign
- Calcium stabilizes the heart
- Insulin shifts potassium into cells
- Dialysis removes potassium
- Sine wave = pre-arrest rhythm
- Treat ECG changes immediately
If potassium is elevated with ECG changes, this is an emergency.
Integrating Hyperkalemia Recognition into Nursing Practice
For every nurse and experienced RN nurse, hyperkalemia management requires rapid assessment, rhythm interpretation, and decisive intervention.
Mastering ECG progression strengthens:
- Telemetry interpretation
- Critical care response
- Dialysis nursing skills
- Emergency preparedness
- NCLEX performance
This knowledge saves lives daily in acute care settings.
Final Thoughts
Hyperkalemia is not just a lab abnormality — it is an electrical emergency. ECG progression from peaked T waves to sine wave rhythm can occur quickly and without warning.
For every registered nurse, understanding this progression and implementing a structured nursing bundle ensures safe, evidence-based care and confident NCLEX readiness.
Recognize early. Act fast. Protect the heart.